





















Introduction
Diabetic macular edema (DME) is a vision-threatening disease that can cause moderate to severe, and even permanent, vision loss. Globally, 285 million people were estimated to be visually impaired in 2010, with 39 million completely blind.96 21 million people were estimated in 2010 to live with DME worldwide.20
Not only does vision loss drastically impede on the ability to live an independent high-quality life, its widespread prevalence also imposes a social and economic burden on individuals, communities and governments.97
DME develops from an eye condition called diabetic retinopathy, which is a complication of type 1 and type 2 diabetes. Approximately 11% of diabetes patients currently have DME, and prevalence increases with the duration of diabetes.97 In order to understand DME, we must first understand diabetes and diabetic retinopathy.
Diabetes

Diabetes can develop if the pancreas does not produce a sufficient amount of insulin, or if the body’s cells are not able to react adequately to the insulin produced by the pancreas. This leads to a high level of blood glucose (blood sugar), which may cause severe consequences, including vascular complications, organ failure or even premature death.2
Diabetes is a chronic disease for which there is currently no cure available. However, a series of therapy options can help to effectively improve quality of life for patients. For these therapies to be successful, self-management of the patient is essential. Diabetes self-care requires a high level of support and motivation by the doctor, the patient’s friends and relatives, and thorough information to help achieve a successful therapy.
The International Diabetes Federation (IDF) estimates that 382 million people are living with diabetes worldwide7.
Diabetes: Type 1 and 2
Type 1
In type 1 diabetes, the cells of the pancreas, which secrete the insulin, are erroneously identified by the immune system as alien and are destroyed.12 People with this disease do not produce any insulin and need a lifelong administration of the hormone by injection or a pump. Type 1 diabetes can develop at any age, but is most frequently diagnosed in children and young adults. Despite many modern, medical achievements and a consequent therapy, diabetes related damages might occur due to other uncontrollable circumstances. Patients with type 1 make up only 5% of all diabetes cases, however, 98% of patients with type 1 diabetes develop a form of diabetic retinopathy after 15 years or more.14
Type 2
In type 2 diabetes, either the body no longer produces enough insulin,2 or the body’s cells no longer react effectively towards the insulin.12 Thus, glucose accumulates in the blood instead of being taken up into the cells.12 A chronically elevated blood glucose level may lead to an array of health complications,11 which could include blindness due to a diabetic eye disease. 78% of patients with type 2 diabetes suffer from a form of retinopathy. When type 2 diabetes is first diagnosed, many patients already show signs of retinopathy, this is because the disease often remains undiscovered for a long period of time. 14 Risk factors for type 2 diabetes include genes, a sedentary lifestyle, smoking, and an unhealthy and highly caloric diet. Measures to take against type 2 diabetes include a healthy diet, an active lifestyle, appropriate use of prescribed drugs, and the application of insulin. Additionally, high blood pressure has to be treated. A change in lifestyle is a big challenge for patients. Doctors, diabetes counselors, friends and relatives can contribute a great deal to improve the course of diabetes through support and motivation.
It is important to remember that for all kinds of diabetes, even with a faithful therapy by the patient, diabetes related complications might occur. With modern therapies, however, complications in the eye can often be treated successfully. A prerequisite is a timely diagnosis, which can be achieved by having regular preventive medical examinations.
Complications
Diabetes can lead to a range of health complications, such as blindness, high blood pressure, kidney disease, neuropathy (nervous system disease), heart disease, stroke, and amputation.3
Blindness can be caused by a number of eye complications known as diabetic eye disease.
Major Areas of the Body Affected by Diabetes
Diabetes can affect almost the entire body. The high build-up of glucose in the blood can lead to a number of complications affecting anything from the eyes to the feet. Controlling your blood glucose levels can help to prevent or manage such complications.
This image highlights the most common parts of the body affected by diabetes.
Diabetic Eye Disease
Diabetic eye disease represents a number of eye conditions that diabetes patients may develop as a complication of diabetes, including diabetic retinopathy and diabetic macular edema. Both of these conditions can cause vision loss or blindness.15
Diabetic Retinopathy
Diabetic retinopathy (DR) is the most common diabetic eye disease and the leading cause of blindness among working adults around the world.7 Anyone with type 1 or type 2 diabetes is at risk15 and should get a dilated eye exam every year to test for DR. Diabetic macular edema can occur at any point in the progression of diabetic retinopathy.15
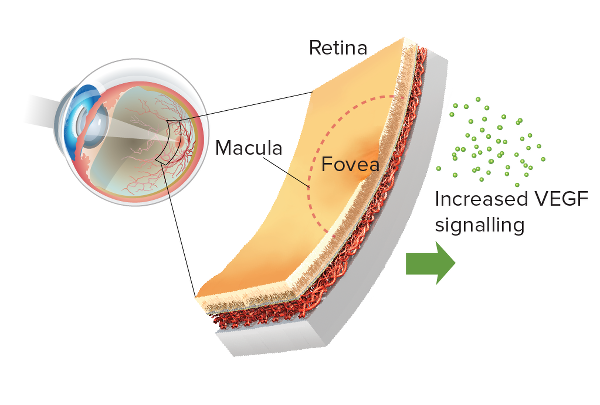
Diabetic retinopathy is a disorder of the retina that occurs when retinal blood vessels are damaged as a complication of diabetes. The retina is the tissue at the back of the eye17 that receives what you see and sends signals to your brain. A small part of the retina, called the macula, is critical for seeing fine details clearly.13

Prevalence
Diabetic retinopathy affects approximately 93 million people worldwide as of 2010.20 Global estimates in 2010 found that a third of people with diabetes have signs of diabetic retinopathy.19
Development of Diabetic Retinopathy
In people with diabetes, elevated blood glucose levels in the retina cause damage and swelling to the retinal blood vessels.23 This may deprive the retina of needed oxygen (a condition called hypoxia), which causes an increase in levels of the glycoprotein VEGF (vascular endothelial growth factor). High levels of VEGF in the retina increase vascular permeability and weaken retinal blood vessels, which contributes to blood vessels becoming leaky.
When blood vessels leak fluid into the retina, the retina swells and vision becomes blurry. If left untreated, this can lead to severe vision loss. In most cases, diabetic retinopathy affects both eyes.54
There are two types of diabetic retinopathy:
1) Nonproliferative Diabetic Retinopathy (NPDR)
The most common form of retinopathy, this condition occurs when tiny blood vessels in the retina swell and form pouches, or microaneurysms, that begin to block blood vessels in the retina. As more blood vessels become blocked, nonproliferative retinopathy progresses from mild to moderate and severe stages.13
2) Proliferative Diabetic Retinopathy (PDR)
This is the most serious stage of retinopathy. It may take several years to develop. In the proliferative stage, the retina cannot receive enough nutrients or oxygen from the damaged blood vessels so it sends signals to nearby tissue for growth of new blood vessels (neovascularization) for nourishment. This increases VEGF levels enough to stimulate growth of new blood vessels. However, these new vessels are fragile and break easily. When they break, fluid and blood leak into the retina, blur vision and, if left untreated, cause severe vision loss.13, 77
Stages
Diabetic retinopathy develops in four stages.15 DME can develop at any stage, though it is more common in the advanced stages.24
Macular edema can develop silently (without symptoms) at any of the four stages of diabetic retinopathy,15 though it is more common in the later stages.24
Diabetic Macular Edema
Diabetic macular edema (DME) is a form of diabetic retinopathy and a leading cause of vision loss in patients with DR.26, 27 It is characterized by swelling or thickening of the retina and the leaking of fluid, specifically in the macula,28 a small area in the back of the eye that focuses and sharpens vision.15

Prevalence
Globally, 21 million people are estimated to live with DME.20 Over 20% of people living with type 1 diabetes and 14-25% of people with type 2 diabetes (depending on their use of insulin) will develop DME within ten years.29, 30
Development of DME
DME is caused when fluid accumulates in the macula. It can develop without symptoms at any of the four stages of diabetic retinopathy, though it typically occurs in the more advanced forms. It is found in almost 50% of people with proliferative retinopathy, the advanced stage of DR.15
As was described in the development of diabetic retinopathy, high levels of blood glucose in diabetes patients cause damage to retinal blood vessels. This may deprive the retina of needed oxygen (a condition called hypoxia), which prompts an increase, or upregulation, in the glycoprotein VEGF (vascular endothelial growth factor). High levels of VEGF weaken the vessel wall and increase vascular permeability, which contributes to blood vessels becoming leaky.
As the vessels leak fluid and blood into the retina and, ultimately, the macula, the macula swells and thickens, resulting in macular edema.15
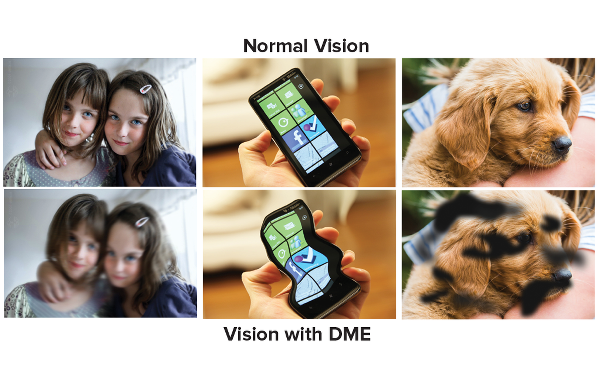
Swelling of the macula reduces visual acuity,31 the clarity or sharpness of vision at a distance, and blurs sight. If left untreated, DME can lead to severe and even permanent vision loss. When DME is treated in its early stages, vision loss can be delayed, stopped or, in some cases, even reversed.13

DME: TWO TYPES
There are two types of diabetic macular edema: focal and diffuse. However, there is no clear, consistent definition for these two types, and the classification and use of these terms has been inconsistent.32 It can be helpful to distinguish between focal and diffuse forms of DME because they may have different pathological processes, which would affect prognosis and predicting treatment outcomes24 for some therapies.
Focal
Focal macular edema is the most common and less severe form of DME.32 It is caused by changes in the structure of the retinal blood vessels, such as microaneurysms33 or dilated capilleries,32, 34 that leak fluid into a smaller area of the macula and do not involve the center of the macula.32 Because edema is limited, visual acuity does not decrease as much as it does in the diffuse form.
Diffuse
Diffuse macular edema is a less common but more severe form of DME that can be difficult to manage.24 It occurs when small capillaries in and around the macula leak fluid throughout most of the macula,34 including its center.32 As a result, most of the macula is thickened and visual acuity is more greatly reduced.32 The risk of developing diffuse macular edema increases with the severity of diabetic retinopathy.28
Risk Factors: Diabetic Retinopathy & DME
A risk factor is anything that affects your chances of getting a disease. Research has focused on risk factors for diabetic retinopathy so there has been little examination of risk factors specific to DME.24 However, diabetic retinopathy and DME both develop as a complication of diabetes and have similar risk factors.
If you have diabetes, you should get a comprehensive dilated eye exam every year. See the Testing section for more info.
(High levels of blood glucose)
Studies have shown that keeping glycemic levels as close to normal as possible can delay or prevent the development of DR.6, 39, 40, 41
(Abnormal levels of blood lipids)
(High blood pressure)
Hypertension-associated end-organ damage is a risk factor specific to DME.35
(Kidney disease)
Addressing the risk factors is the best way to slow or halt progression of either disease, which may occur without any changes to vision until it is too late to treat the condition. Diabetic retinopathy and DME rarely have visual symptoms in their early development and vision loss can occur very suddenly, so it is important to get regular screenings before symptoms appear.13
Monitoring & Symptoms
Diabetic retinopathy develops without early symptoms or causing pain.15 Even in the advanced stages, proliferative retinopathy may not cause symptoms.15 Macular edema can develop at any stage of diabetic retinopathy without affecting vision.15 It is important not to wait for symptoms. Get tested before any issues with vision occur.
If blood vessels bleed into the eye, you may see blind spots in your vision. The spots may clear temporarily, but bleeding may reoccur and damage vision if the condition is left untreated. You may also experience blurry vision, or colors may look “washed out” or faded.55 Go see an eye care professional at the first sign of any of these symptoms.

In its early stages, diabetic retinopathy can be treated and vision can be preserved.19 If you do not receive treatment, diabetic retinopathy may progress into the proliferative form. Macular edema can also develop without symptoms and, if timely treatment is not obtained, DME may result in severe vision loss.
Early detection and timely treatment can save your vision. Learn How:
What You Can Do
As a person with diabetes, regular maintenance and regulation of your condition should be an integral part of daily life. There are steps that you can take to prevent or delay vision loss, and manage your condition and treatment:56
-
Regular Screening:
Get a comprehensive dilated eye exam at least once a year.It is recommended that people aged ten years or older with type 1 diabetes have a comprehensive eye exam within five years of the diagnosis, and that people with type 2 diabetes get a comprehensive eye exam as soon as they are diagnosed. Both type 1 and 2 diabetes patients should continue to receive subsequent eye exams on an annual basis.15,16 Less frequent exams may be an option after successful completion of one or more normal eye exams. If diabetic retinopathy is progressing, exams may be more frequent.16
Work with your eye care specialist to assess the best frequency of exams in order to manage your condition and prevent, or slow down, disease progression.
-
Control Blood Glucose:
HbA1c levels are a long-term measure of blood glucose control. HbA1c is a molecule that is formed when hemoglobin, a protein in red blood cells, connects to glucose.37 If there is more glucose in the blood to connect with hemoglobin, then more HbA1c will form.Keep your blood glucose levels as close to normal as you can.1 Hyperglycemia initiates many other risk factors, so controlling blood glucose can prevent other diabetic complications and slows down or even prevents the development of retinopathy.15
Discuss with your doctor about how best to control blood glucose levels.
-
Control Blood Pressure:
Studies have demonstrated that keeping your blood pressure as close to normal as possible reduces the risk of complications in the microvascular system by roughly 33%.1
Typically, the goal is to maintain a consistent blood pressure < 130/80 or below the 90th percentile for age, sex, and height (whichever number is lower).16
You can find more information on healthy blood pressure levels specific to age, sex and height at: www.nhlbi.nih.gov/health/prof/heart/hbp/hbp_ped.pdf -
Control Blood Lipids:
Keeping your cholesterol levels as close to normal as possible reduces risk of complications.1 High levels of total cholesterol or triglycerides can increase the risk of developing DME by two- or three-fold.57

Testing
If you have type 1 or type 2 diabetes, you should get a comprehensive eye exam at least once a year to screen for diabetic retinopathy and diabetic macular edema.
An ophthalmologist or optometrist who is experienced in diagnosing, managing and treating DR and DME is best suited to conduct these exams.16
A comprehensive eye exam typically includes a dilated eye exam, visual acuity test and tonometry. These tests can detect early signs of DR or DME, such as:15
- Retinal blood vessels that leak
- Damage or any change to the blood vessels
- Swelling or thickening of the retina

Types of Tests
A comprehensive eye exam includes:
1. Dilated Eye Exam
During a dilated eye exam, you will receive eye drops that dilate your pupils. This allows your eye specialist to see what is happening inside your eyes. Using a magnifying lens, your eye specialist will assess your retina and optic nerve to find any potential problems. If you have diabetes, it is important to receive this test at least once a year.15
2. Visual Acuity Test
This test uses an eye chart to measure your vision at various distances.15
3. Tonometry
This test measures the pressure in your eye(s) and may use numbing drops.15
4. Fluorescein angiogram (FA)
This test is taken when presence of DME is suspected. A certain type of dye will be injected into your arm and will pass through your blood vessels. This dye allows pictures to be taken of the retinal blood vessels so your eye care professional can detect any vessels that leak. If DME is found, work with your eye care specialist to determine the best treatment.15
5. Optical Coherence Tomography (OCT)
OCT is another tool that tests for DME. It is a certain type of camera that photographs and measures the thickness of your retina. It is also effective at detecting any swelling and fluid in the retina.58 The benefit of OCT is that it is non-invasive. Also, it makes it possible to evaluate treatment response more objectively.33
When to Get Tested16
Type 1 Diabetes
Patients with type 1 diabetes aged ten years or older should have their first comprehensive dilated eye exam within 5 years of developing diabetes.
Type 2 Diabetes
Patients with type 2 diabetes should have their first comprehensive dilated eye exam as soon as their diabetes is diagnosed.
Both type 1 and 2 diabetes patients should continue to receive subsequent eye exams on an annual basis. Less frequent exams may be an option after successful completion of one or more normal eye exams. Exams will be more frequent if retinopathy is progressing. Work with your ophthalmologist or optometrist to identify the best frequency of testing for you.
If you are diagnosed with severe nonproliferative diabetic retinopathy, proliferative diabetic retinopathy, or DME, go see an eye specialist experienced in treating and managing these conditions.
Understanding VEGF & Macular Edema
What Is VEGF?
The vascular endothelial growth factor (VEGF) is a glycoprotein that has been found to contribute significantly to the development of diabetic macular edema. VEGF plays an important role in many processes in the body, but excessively high levels of VEGF can have harmful effects.
VEGF & DME
Excessively high levels of VEGF have been found in retinopathy59 and DME.61 When retinal blood vessels become weak or blocked in diabetic retinopathy, the retina cannot receive enough blood or oxygen (hypoxia) and sends signals to the body for nourishment. VEGF is then released in the retina at abnormally high levels, which increases vascular permeability. This contributes to the rupture of the blood vessel wall and consequential swelling of the vessels,33, 60 resulting in damaged vessels that leak33 fluid into the central retina. As fluid accumulates in the macula, the macula swells and thickens, resulting in swelling of the macula and, ultimately, DME.
Research has shown that over-expression of VEGF plays a significant role in DME61 and is an important target for treating the condition.
Patient Perspective
Ang-2 Webinar
The Angiogenesis Foundation has published a new Webinar Series on Vascular Stabilization in Retina Health and Disease to provide the vision community and clinicians treating retinal vascular eye diseases with an up to date overview of the Angiopoietin-Tie Pathway, and how this pathway is involved in retinal health and disease.

Webinar speakers include: Max Gomez, PhD, Charles Wykoff MD, PhD, David Eichenbaum, MD, and Ramin Tadayoni, MD, PhD. Watch now: https://www.scienceofang2.org/webinar